Kenya freed suicide from the law, but the weight of shame still lingers, in hospital rooms, in churches, in classrooms, in homes, and across our communities. Why do families still hide the truth? Why do schools turn a blind eye? And why does silence continue to stalk those who are hurting?
When ‘Mary’ woke up in a hospital bed after swallowing a handful of pills, she expected compassion. Instead, she was handcuffed. A police officer stood guard at the door. That was 2023. Two years later, suicide is no longer a crime, but Mary still hasn’t told her family what happened.
This World Suicide Awareness Day 2025, I reflect on an issue that remains stubbornly persistent. Earlier this year, on January 9, 2025, the High Court of Kenya declared Section 226 of the Penal Code unconstitutional, effectively decriminalizing attempted suicide. Justice Lawrence Mugambi ruled that the law violated fundamental rights, including equality, human dignity, and access to healthcare.
The Kenya Psychiatric Association (KPA), co-petitioner in the case, hailed the ruling as a milestone that prioritizes medical care over criminal punishment and encourages open conversations around mental health instead of condemnation.
I looked at this change more closely in my previous article, ‘What’s Next for Kenya? Beyond Suicide Decriminalization’
Nine months later, little has changed on the ground. Despite the legal progress, stigma continues to haunt homes, schools, churches, and communities, leaving many survivors and their families isolated and silenced.
For real change to take root, this conversation must begin with me and you. For the longest time, we’ve believed that true change only begins with policy. But what we don’t always understand is that behind those policies are real people fighting for real change. They can win petitions and legal battles, but unless we support the cause like they do, societal transformation remains almost impossible. Real change, where survivors feel seen, supported, and safe, can only begin with us.
The Stigma Problem
Most of the time, when we talk about challenges facing mental health, stigma is immediately brought into the discussion. Yet, the truth is, stigma is one of the challenges we could begin to eliminate if we collectively decided to. Not unless we don’t really know what stigma is in the first place.
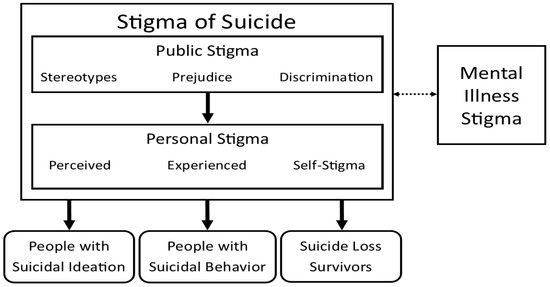
In relation to suicide, stigma continues to persist in more ways than we ever imagine. It is when you judge someone for attempting it before trying to understand what drove them there. It is when your friend confides in you about suicidal thoughts, and instead of listening, you react with shock or discomfort. Stigma is when you feel ashamed or embarrassed after a close family member or friend dies by suicide, as if their death is something to hide or be ashamed of.
Stigma is when you whisper about someone’s struggle behind their back instead of offering support. It is when schools, workplaces, or communities treat survivors as “weak” or “troubled” rather than seeing them as human beings in need of care. Stigma is when religious or cultural teachings frame suicidal thoughts as a moral failing instead of a mental health concern.
Stigma is when a survivor hesitates to seek help because they fear judgment or discrimination. It is when public conversations about suicide are avoided entirely, leaving myths, shame, and silence to thrive. And stigma is much more than this, it sneaks into almost every corner of society, influencing how we think, speak, and act around mental health.
The Psychology of Shame
Stigma persists today because human psychology naturally gravitates toward fear, avoidance, and judgment in the face of uncomfortable realities. Suicide challenges our understanding of life, control, and mortality, creating cognitive dissonance, a mental tension when we confront something we cannot easily explain or manage. Instead of sitting with that discomfort, many people resort to blame, silence, or moral judgment, projecting fears onto those already suffering.
Carson Anekeya
Social conditioning reinforces this: from childhood, we are taught to view suicide as shameful or sinful, and these deeply ingrained beliefs shape our emotional responses long into adulthood.
As a result, even when laws change, the mental scripts we carry about suicide remain hardwired, influencing how we react to survivors, families, and communities.
Beyond individual psychology, stigma is sustained by collective social behavior. Humans are wired to seek safety in conformity, and communities often respond to suicide with secrecy, gossip, or ostracism to protect reputation and maintain social norms. This creates an environment where survivors feel unsafe to speak, families hide struggles, and conversations about mental health are avoided.
Psychologically, the shame survivors internalize can trigger self-stigmatization, where they believe their suffering is a personal moral failing rather than a symptom of psychological distress.
This internalization intensifies isolation, discourages help-seeking, and perpetuates a cycle in which stigma feeds silence, and silence strengthens stigma, a cycle that continues despite legal reforms.
Religious & Cultural Barriers
For the longest time, our cultural and religious circles, our primary sources of identity, have perpetuated stigma around suicide. We may pretend it’s not happening, yet we all know it does. Within many faith communities, suicide is often framed as a sin, a moral weakness, or even a form of divine punishment. This moral framing places blame on the individual rather than recognizing the mental health struggles that led them there, pushing survivors into silence and shame.
Cultural expectations compound this problem. Families feel pressure to maintain honor and protect their reputation, often hiding suicide attempts or deaths to avoid gossip or public judgment. This secrecy creates a cycle of silence, where neither survivors nor grieving families feel safe to speak about their experiences or seek help. Religious rituals and mourning practices can also unintentionally stigmatize victims, funeral rites may exclude those who died by suicide, and community ceremonies may treat the death as dishonorable. The psychological impact: survivors may internalize guilt and shame, while grieving families experience compounded grief, isolation, and fear of judgment.
Survivors and their families often choose silence, not because they want to, but because speaking out risks condemnation from faith leaders or community members.
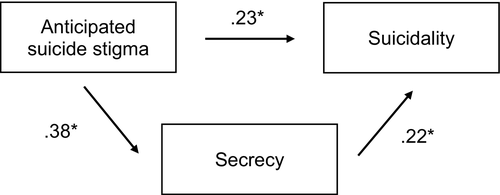
A 2020 study “Anticipated Suicide Stigma, Secrecy, and Suicidality Among Suicide Attempt Survivors” by Mayer and colleagues sheds light on how this silence and stigma deepen the wound for suicide attempt survivors. Their model showed that anticipated stigma was directly linked to higher suicidality (.23*), but it also worked indirectly by fueling secrecy (.38*), which in turn increased suicidality (.22*).
The researchers found that when survivors anticipate being judged or shamed, they are more likely to keep their experiences secret, and this secrecy directly increases the risk of ongoing suicidality. In other words, the very fear of stigma not only silences survivors but also traps them in cycles of isolation and distress. For families, this means that the pressure to hide suicide attempts or deaths does not protect their loved ones; instead, it reinforces suffering and cuts off pathways to healing and support.
Recently, many survivors have shared how they’ve been “church hurt” experiencing judgment, condemnation, or dismissal from faith communities when they sought support. Some have even left their churches entirely, unable to reconcile the message of hope with the shame and criticism they faced. It is a reminder that while faith communities have the potential to be pillars of support, they can also perpetuate stigma if they fail to respond with empathy and understanding.
It is high time churches become primary points of support for those struggling with suicidal thoughts or mental health challenges. Just as they preach hope, they can actively bridge the gap between spiritual guidance and mental health care. It has been promising to witness some faith communities stepping into this role. For example, a feature I recently explored, “Faith in Healing: How Trinity Chapel Ruiru is Bridging Kenya’s Mental Health Gap,” this church has created safe spaces, counseling programs, and mental health awareness initiatives that support vulnerable members of their congregation. Other churches across Kenya can emulate such efforts, positioning themselves not only as spiritual centers but as beacons of hope and practical support in the fight against stigma in society.
Lived Realities: Voices from the Ground
From a brief study I conducted, responses from different groups revealed consistent patterns about how stigma continues to shape experiences after suicide attempts, even nine months after the law decriminalized it.
Survivors reflected on the tension between legal progress and social judgment:
“Since the law decriminalizing suicide was passed, some people have been more understanding, but much of the judgment remains. Walking through my village, I’ve overheard children asking why my mother tried to kill herself. The law changed, but the whispers and stares didn’t disappear. Sometimes, I feel safer sharing my story with friends online than with people around me.”
Family members highlighted the ongoing social scrutiny that accompanies a suicide attempt or death:
“After my brother attempted suicide, our family faced a lot of gossip. Even after the law changed, neighbors still avoided us or whispered behind our backs. People talk about mental health more now, but mostly in general terms, they rarely discuss it openly in a way that supports families going through it. It feels like the law gave us a shield, but not acceptance.”
Mental health advocates and counselors noted increased help-seeking but persistent barriers:
“Since the decriminalization, we’ve noticed an increase in calls to our helpline, but many survivors still hesitate to reach out. Fear of exposure, judgment from family or community, and cultural shame are huge barriers. Legal change is only the first step; without community awareness and empathy, survivors still face walls of silence and stigma.”
Community members and religious leaders emphasized the need for education and safe spaces:
“Communities need education and safe spaces where people can speak freely about mental health. Survivors should feel supported, not blamed. There’s a big gap between legal progress and societal acceptance, many still view suicide as a moral failing. Religious and community leaders can bridge that gap, but it requires courage and openness to challenge long-held cultural beliefs.”
Finally, respondents reflected on the personal impact of stigma:
“I remember when a close friend attempted suicide a few years ago. People whispered, avoided him, and even his family seemed ashamed. He stopped talking about his feelings entirely. That experience taught me that stigma is more damaging than the act itself, shame isolates, fear silences, and for many, the world feels unsafe even after surviving. This is often why subsequent attempts occur.”
Changing the Narrative on Suicide

World Suicide Prevention Day 2025 reminds us that the conversation around suicide must shift from blame and stigma to empathy and understanding. Legal reforms alone cannot protect those at risk, society must change how it talks about suicide, reframing it as a public health issue and a human experience rather than a moral failing. Families, friends, schools, and faith communities must actively participate in reshaping narratives, creating environments where survivors feel safe to share, grieve, and seek help without fear of judgment.
Carson Anekeya
Changing the narrative requires education, visibility, and proactive support. Communities can host workshops, awareness campaigns, and storytelling initiatives that highlight lived experiences, dismantling myths and fears that fuel stigma. Mental health professionals, peer support groups, and advocacy organizations must be amplified so that every survivor knows there is a network ready to listen, guide, and heal. When society validates vulnerability instead of condemning it, we empower individuals to seek help before crises escalate.
Finally, the narrative shift starts with each of us. By speaking openly, challenging harmful assumptions, and prioritizing compassion over gossip or judgment, we collectively redefine what it means to support those struggling with suicidal thoughts. On this World Suicide Prevention Day 2025, let us commit to transforming silence into dialogue, fear into empathy, and shame into solidarity, because changing the narrative is the first step toward saving lives.
- The Rise of Suicide Posts in Digital Spaces Reflects a Growing Mental Health Crisis - February 22, 2026
- How Kenya’s Silent Lifestyle Disease Crisis Is Reshaping Public Health - February 12, 2026
- The Rise of Lifestyle Diseases Emerges as a Crisis Among Kenya’s Youth - February 9, 2026