Beyond the 2025–2030 Cervical Cancer Elimination Plan, the pressing question remains: who is accountable for delivering real results for Kenyan women?
On 16 January 2026, the Government of Kenya officially launched the National Cervical Cancer Elimination Action Plan 2025–2030, a five-year strategy developed with support from the World Health Organization (WHO) to accelerate prevention, early detection, and treatment of cervical cancer. The plan aligns with WHO’s global targets to eliminate cervical cancer as a public health problem and is designed to be results-oriented, costed, and inclusive, with a strong focus on equity, quality, and nationwide scale-up.
Cervical cancer remains the second most common cancer among Kenyan women, with an estimated 5,845 new cases and 3,600 deaths annually. Despite being largely preventable through HPV vaccination and early screening, many women continue to be diagnosed at advanced stages due to limited access to services.
Building on Kenya’s national HPV vaccination programme, the country transitioned in November 2025 to a single-dose HPV vaccination schedule, in line with WHO recommendations, to simplify delivery and improve coverage. During this transition, WHO supported the Ministry of Health to train more than 11,000 health workers nationwide, strengthening capacity for vaccine delivery and cervical cancer services. The Action Plan also emphasizes integrating cancer services into primary health care, expanding screening, improving referral systems, and leveraging digital tools, efforts aimed at reaching women across all 47 counties and turning policy commitments into measurable outcomes.
The Promise of a Plan
With every plan comes a sense of hope and vision, a belief that structured action can transform a challenge into a solution. Yet, sometimes that hope can blind us, leaving promises unfulfilled and aspirations unmet. In Kenya, the launch of the 2025–2030 Cervical Cancer Elimination Plan represents such a moment of optimism. Designed to reduce deaths and expand early detection, the five-year strategy signals the country’s commitment to tackling a disease that remains largely preventable but continues to claim thousands of lives each year.
The plan builds on existing initiatives, including HPV vaccination, early screening, and integration of services into primary health care, offering a roadmap to reach women across all 47 counties. But having a plan is one thing, so who will ensure it delivers real results? As we all know, without clear accountability, even the most ambitious strategies risk fading into another chapter of good intentions with limited impact.
Learning from Past Plans
One of the recurring challenges in Kenya’s health sector is that planning often outpaces implementation. Ambitious policies and strategies are developed, but translating them into tangible results has consistently lagged. Without clear accountability, sufficient resources, and strong monitoring systems, even well-designed plans risk failing to deliver meaningful impact on the ground.
Several past initiatives illustrate this persistent implementation gap in concrete ways. The Kenya Health Policy 2014–2030 envisioned universal access to essential health services through devolution, with counties serving as the primary delivery units. However, the policy assumed a level of county readiness that did not exist uniformly. Many counties lacked the fiscal space to prioritize preventive services once health functions were devolved, resulting in recurrent underfunding of screening, community outreach, and health workforce expansion. In addition, the policy did not establish enforceable accountability mechanisms to align national priorities with county Integrated Development Plans (CIDPs), leading to wide disparities in service availability and outcomes across counties.
The Kenya National Cancer Control Strategy 2017–2022 was similarly ambitious, calling for nationwide scale-up of cervical cancer screening, early diagnosis, and referral networks. In practice, implementation faltered because the strategy relied heavily on facility-based screening without adequately addressing workforce shortages, equipment availability, and supply chain constraints at primary and county referral levels. Screening targets were set, but referral pathways for women who screened positive were poorly defined and inconsistently funded, resulting in delayed diagnosis, loss to follow-up, and fragmented care. Data reporting systems for cancer screening and treatment were also weak, limiting the ability to track coverage, outcomes, and accountability for results.
The Kenya Reproductive, Maternal, Newborn, Child and Adolescent Health (RMNCAH) Investment Framework 2016–2030, together with the Newborn, Child and Adolescent Health (NCAH) Policy 2018, explicitly promoted the integration of preventive services into routine maternal and reproductive health care. These policy instruments positioned antenatal, postnatal, and family planning visits as critical entry points for preventive interventions, including cervical cancer screening. However, implementation proved uneven across counties, with many county health systems lacking the human resources, essential commodities, and supervision structures required to operationalize integrated service delivery at scale.
In practice, overstretched health workers were often compelled to prioritize acute and curative maternal services, leaving preventive interventions under-resourced. Budget allocations at county level frequently favored visible infrastructure and emergency care over screening and follow-up services, while monitoring frameworks focused more heavily on maternal mortality and service utilization than on preventive coverage indicators. As a result, community-level demand creation and follow-up for preventive services remained weak, particularly in rural and marginalized counties, limiting the reach and effectiveness of these plans despite their strong policy intent.
Kenya has no shortage of plans, but the real challenge lies in execution and accountability. When plans fail to translate into action, it is often the people of Kenya who suffer the consequences. Delays in implementation can make it nearly impossible to recover lost momentum, and three years into a plan, efforts to form ad-hoc committees or salvage progress cannot fully undo the damage. To protect lives and achieve meaningful results, accountability and follow-through must be built into the system from the very start.
Why Plans Often Fail Before They Start
First, policy-driven approaches often fail because we continue to develop comprehensive plans, yet weak accountability mechanisms, inconsistent financing, and limited follow-through at county and facility levels undermine implementation. Even the most well-designed strategies cannot succeed when resources and oversight are not aligned with the plan’s goals.
Second, accountability suffers when responsibility for delivery is diffused. Without clear ownership, measurable targets, and consequences for inaction, progress stalls long before a plan can make a tangible difference.
Finally, advocacy-focused promises frequently fall short. Women are assured access through national plans, yet delays in rollout, workforce shortages, and uneven county commitment mean that many of these commitments are never fully realized, leaving women without timely, lifesaving services.
Current Gaps in the 2026–2030 Plan
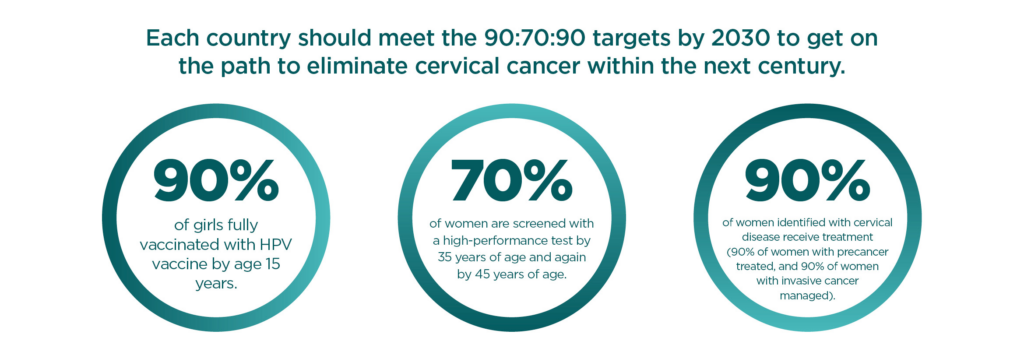
While Kenya’s National Cervical Cancer Elimination Action Plan (2025–2030) sets ambitious targets aligned with the WHO’s global 90-70-90 goals for vaccination, screening, and treatment, several structural and implementation limitations could weaken its impact.
The plan’s official launch documents describe priorities, such as expanding HPV vaccination coverage, scaling up HPV DNA testing and self-sampling, strengthening referral systems, building workforce capacity, and leveraging digital health innovations, but they provide limited detail on how accountability, financing, and monitoring mechanisms will work in practice.
First, governance and accountability mechanisms are not clearly articulated in publicly available summaries of the plan, which focus on what interventions are prioritized but offer less clarity on who is responsible for delivering, monitoring, and reporting on results at national, county, and facility levels. There is a risk that implementation could follow patterns seen in prior strategies where responsibility becomes diffused. This gap means that weak accountability structures could slow progress or result in uneven action across counties.
Second, financing remains a potential barrier. While the plan is described as “costed and results-oriented,” there is little publicly available detail about how much specific components will be funded, how resources will be tracked, or whether counties will have dedicated budgets for scaled-up activities like HPV DNA testing, self-sampling distribution, data systems, and digital tools. Independent analyses conducted during the plan’s development identified persistent financing gaps in Kenya’s cervical cancer programme. These include an overreliance on donor support, low county-level budget allocations for preventive services, and challenges in health insurance coverage that limit sustained investment in screening, treatment, and follow-up services.
Third, the plan’s design calls for expanded use of digital health tools to extend services to women across all 47 counties, but publicly available summaries provide few specifics on how these technologies will be deployed, resourced, or integrated into existing health information systems. Kenya continues to celebrate its embrace of innovation, self-screening kits, artificial intelligence–supported diagnostics, digital referral platforms, and mobile clinics, but a critical question remains: are these innovations reaching the women who need them most?
For example, a 2025 study tested AI-supported cervical cancer screening in Kenya and Tanzania by digitizing samples and analyzing them with machine learning at rural hospitals, showing potential but also highlighting that without investments in trained staff, equipment, and community trust, such technologies cannot reach their full impact.
Evidence from such studies consistently shows that women in rural and low-resource settings remain disadvantaged by limited connectivity, weak facility capacity, and uneven rollout of new technologies. As a result, the promise of digital health risks outpacing reality, widening rather than closing equity gaps unless deliberate investment is made in where and how these tools are used, who they reach, and who is still left out.
Addressing Barriers and Strengthening Implementation
Addressing the persistent gaps in cervical cancer prevention and care will require deliberate, practical action across all levels of the health system. Clear assignment of responsibility is key, with defined roles for national leadership, county governments, and health facilities to avoid the diffusion of accountability that has undermined past strategies. This must be matched with consistent and predictable funding, ensuring that screening, treatment, referral, and follow-up services are adequately resourced in county budgets rather than dependent on short-term projects. Equally important are robust monitoring and reporting systems that track progress beyond coverage targets to include follow-up, treatment completion, and equity of access across regions and populations.
At the same time, implementation must reflect the realities on the ground. Policies and plans can only deliver results if they are designed and executed with the active involvement of frontline health workers, community leaders, and the women they are meant to serve. Community engagement and sustained awareness efforts are critical to building trust, dispelling myths, and increasing screening uptake, particularly in underserved areas. Bridging the gap between planning and real-world impact requires moving beyond policy launch moments to continuous follow-through, learning, and adaptation, we should try and have these plans and policies meet the people where they are.
“Kenya has no shortage of plans, the real challenge lies in implementation and accountability. The gap is in execution. Policies exist, but results depend on who delivers and who is held accountable.”
Carson Anekeya
Cervical cancer is preventable, but too many women are still dying because screening and treatment are not reaching them in time. The 2025–2030 plan sets clear goals, vaccination, screening, treatment, but these will only succeed if someone takes responsibility, if counties are properly funded, and if health workers and communities are fully supported. Policymakers, health workers, and advocacy groups must step up, ensure the plan reaches every woman, and turn these promises into real, lifesaving action.
- The Rise of Suicide Posts in Digital Spaces Reflects a Growing Mental Health Crisis - February 22, 2026
- How Kenya’s Silent Lifestyle Disease Crisis Is Reshaping Public Health - February 12, 2026
- The Rise of Lifestyle Diseases Emerges as a Crisis Among Kenya’s Youth - February 9, 2026